2009-2014 Clinical Medicine, Qilu Medical College, Shandong University
2014-2019 Master and PhD Program in Neurology, Qilu Medical College, Shandong University
From 2019 to present, Department of Neurology, Shandong University Second Hospital, engaged in cerebrovascular disease diagnosis and treatment, and cerebrovascular intervention related work
Published a total of 8 SCI articles as the first author and corresponding author
Participated in 5 national and provincial projects
Case Information
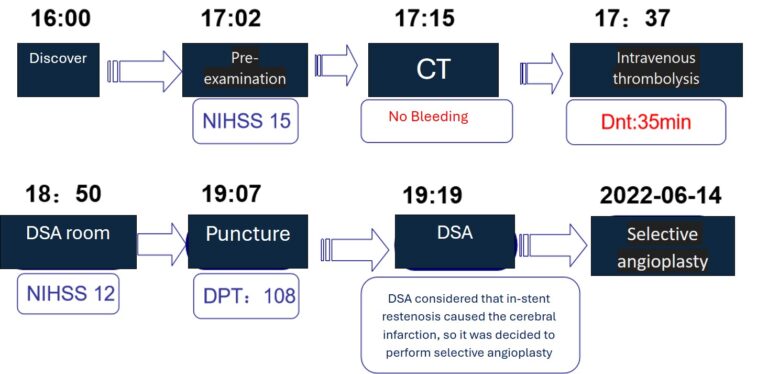
Chief complaint: Found unable to speak, right-sided limb weakness for 2.5 hours. Present illness: On that day at 16:00, the patient was found unable to speak and had right-sided limb weakness by family members. The patient could open eyes upon being called, no obvious vomiting, no urinary or fecal incontinence. Family members immediately called 120 for emergency treatment. Physical examination in the emergency department showed right-sided limb muscle strength at grade 0, unable to speak. Cranial CT showed multiple lacunar infarctions, brain atrophy, suggestive of acute cerebral infarction. The patient was last known to be normal around 13:00, within the intravenous thrombolysis time window, with indications for intravenous thrombolysis and no absolute contraindications. The condition was explained to the family members. After family members signed the consent form, the patient received alteplase thrombolysis (17:37 alteplase 7.2 mg intravenous push, followed by 64.8 mg intravenous infusion). After thrombolysis, there was no significant improvement in muscle strength. After bridging arterial thrombectomy treatment was explained to family members, they signed the consent form for emergency cerebral angiography for arterial thrombectomy. Past medical history: Had left internal carotid artery stenting 6 years ago; history of diabetes for more than 10 years, usually controlled with subcutaneous injection of Mixtard 30/70 and oral metformin; history of hyperuricemia, renal insufficiency, usually taking febuxostat, benzbromarone capsules, compound ammonium chloride tablets, furosemide, spironolactone. Physical examination: NIHSS score 15, GCS score 7 (2+2+3), comatose, unable to cooperate during body examination, eyes deviated to the right, present light reflex, low muscle tone, unable to cooperate during muscle strength examination, slight flexion of limbs seen with painful stimuli, positive Babinski sign on the right side, other parts of the examination were unable to cooperate .
Diagnosis
Acute ischemic stroke
Post left internal carotid artery stenting
Type 2 diabetes mellitus
Hyperuricemia
Renal insufficiency
Treatment Process (AIS Case)
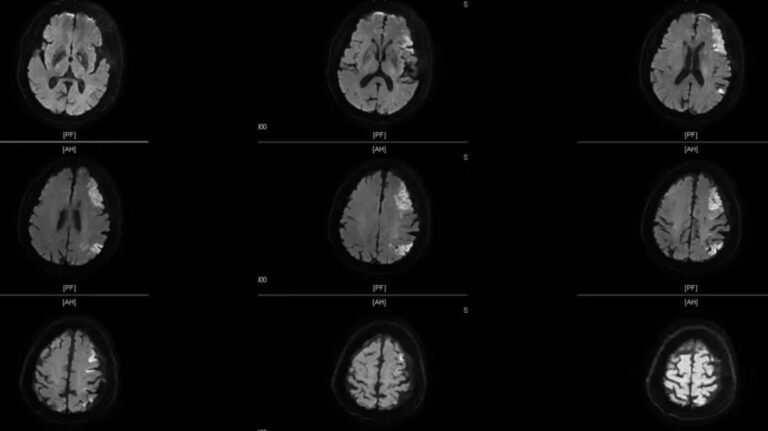
Preoperative Imaging
Cranial MRI DWI: Acute or subacute cerebral infarction in the right pons, left frontotemporal lobe.
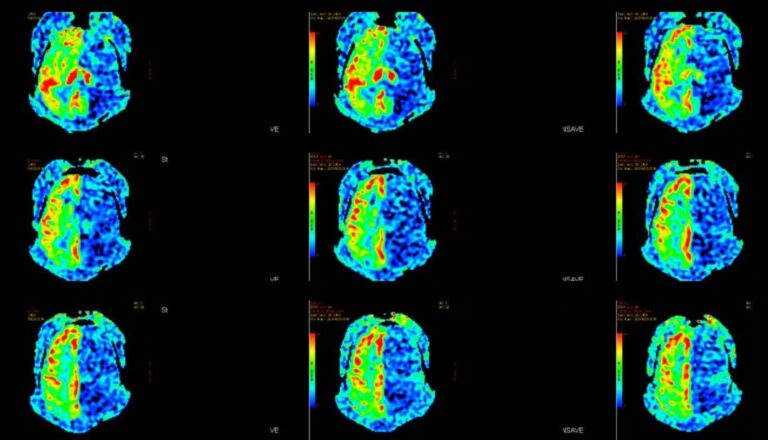
Cranial MRI ASL: Left cerebral hemisphere blood perfusion significantly decreased compared to the right side.
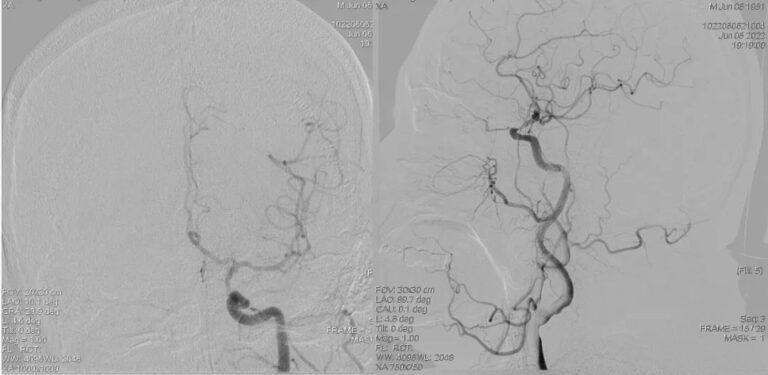
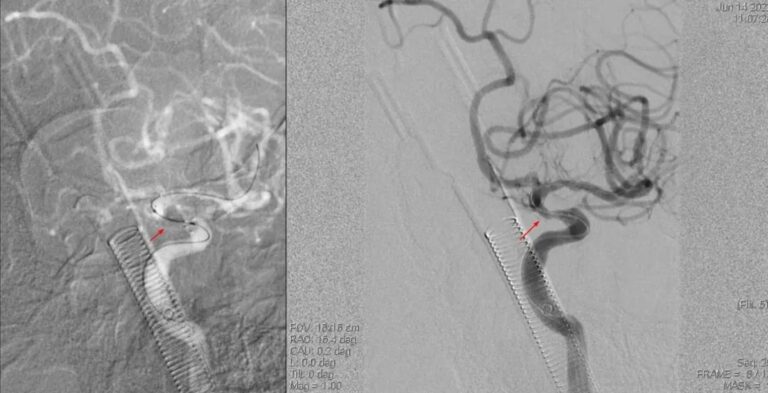
DSA: Severe stenosis at the proximal end of the left internal carotid artery stent in the siphon segment.
Surgical Procedure
Hemo EmerAX / TracLine™ LDP 8F intermediate catheter advanced to the beginning of the C3 segment of the left ICA
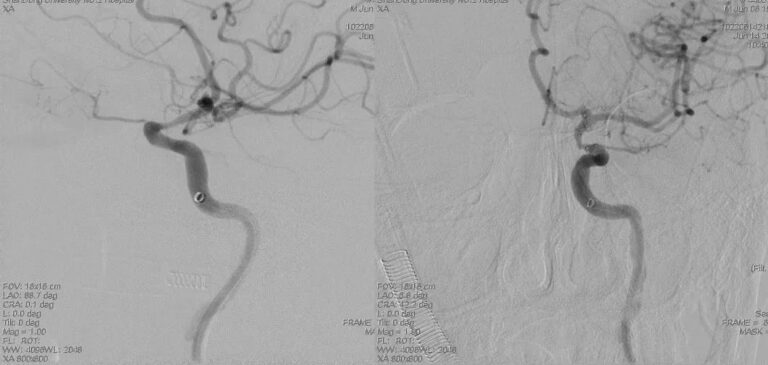
Advanced along the micro-guidewire into the Hemo FocuStar™ 1.5*12mm intracranial balloon dilation catheter, covering the stenotic segment. The stenotic segment was dilated at a pressure of 6 atm, resulting in slight improvement of the luminal narrowing compared to before dilation.
Advanced along the micro-guidewire into the HeMo FocuStar™ 2.5*12mm intracranial balloon dilation catheter, covering the stenotic segment. The stenotic segment was dilated at a pressure of 4 atm, resulting in obvious improvement of the luminal narrowing compared to before dilation. Approximately 40% residual stenosis remains, with no signs of dissection, bleeding, or distal vascular embolization
The narrowing within the stent has significantly improved compared to before, with approximately 40% residual stenosis. There are no signs of dissection, bleeding, or distal vascular embolization.
Postoperative Imaging
Cranial MRI DWI: Acute or subacute infarction in the left parietal lobe.
Cranial MRI ASL: Reduced blood flow perfusion in the left cerebral hemisphere compared to the right, showing improvement compared to preoperative status.
Postoperative Follow Up
The patient is conscious with slightly unclear speech and slightly delayed responses.
Muscle strength in the right limbs is at level V-.
No other significant positive signs were noted on neurological examination.
Case Summary
◐ Case Characteristics:
The patient presented with acute onset symptoms, and post-thrombolysis bridging DSA revealed severe stenosis at the proximal end of the left internal carotid artery stent.
◐ Preoperative Assessment Key Points:
Complete blood count, liver and kidney function tests, biochemistry, cardiac function evaluation, cranial MRI (DWI/ASL/SWI).
◐ Surgical Technique Key Points:
The main technical challenge of the stent restenosis balloon dilatation procedure is to locate and confirm the true lumen of the vessel. The HeMo TracLine™ LDP 8F intermediate catheter has the advantage of high-positioning, can be advanced to the C3 segment of the internal carotid artery, provides good support for the guidewire, can save intraoperative consumables, and is safe in the restenosis balloon dilatation procedure.
Surgical Guidance
Lu Wei Shandong University Second Hospital
Doctor of Medicine, Associate Chief Physician, currently serving as the head of the Neurology Interventional Group at the Second Hospital of Shandong University.
Deputy Director of the Neurointerventional Branch of the Shandong Province Association for Prevention and Treatment of Cerebrovascular Diseases.
Standing Committee Member of the Neurointerventional Professional Committee of the Shandong Medical Association.
Standing Committee Member of the Neurology Interventional Physicians Branch of the Shandong Medical Association.
Standing Committee Member of the Neurointerventional Branch of the Shandong Stroke Society.
Committee Member of the Medical Appraisal Branch of the Shandong Medical Association.
Product
The TracLine™ intermediate catheter boasts several advantages:
1. The 8F TracLine™, as an LDP (Large Lumen Distal Pathway) platform, exhibits excellent navigability, enabling passage through complex anatomical structures to reach the cavernous sinus or beyond.
2. The unique large bore tip design of the 8F TracLine™ provides a larger surface area for thrombus contact, enhancing thrombus aspiration efficiency in the internal carotid artery.
3. With a large inner lumen of 0.088″, it is compatible with multiple instruments, allowing for more options during bleeding and ischemic surgeries.
In July 2021, HeMo Corporation officially released the FocuStar™ intracranial balloon dilation catheter. This rapid exchange (Rx) product offers the following advantages:
1. It has a smaller outer diameter for improved navigability, coupled with a special hydrophilic coating to reduce friction, resulting in excellent product passage.
2. With a nominal pressure of 4 atm, it ensures effective dilation while minimizing the potential risk of vascular damage.
Cookies
Please note that your use of this website is governed by your acceptance of our Terms of Use. We also use cookies on our website to understand the usage patterns of visitors, so that we may be able to enhance their browsing experience and improve the website and/or our services. We may also allow certain third parties to place cookies on our website to collect information about your online activities on our website and across different websites you visit over time. Please click here for more information about our Cookie Policy.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.